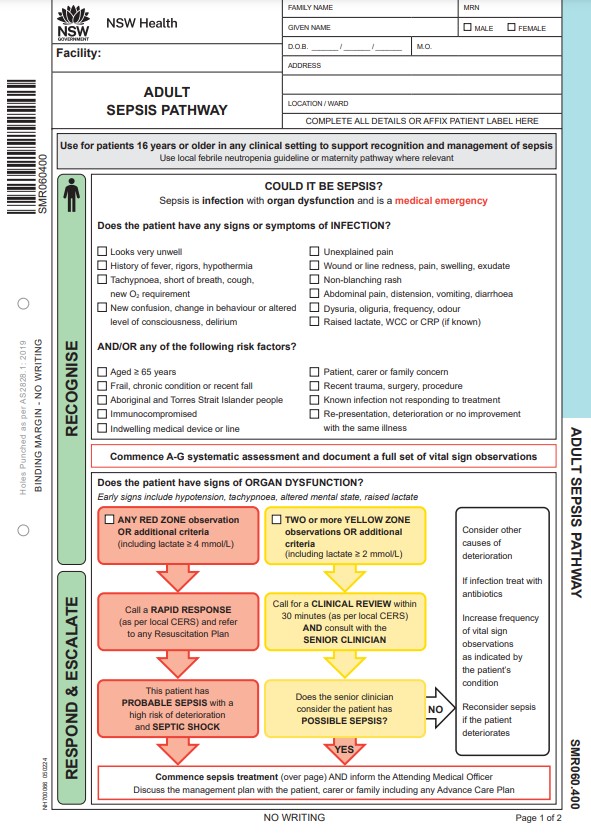
Any person, 16 years and over, presenting with symptoms that fulfil Adult Sepsis Pathway criteria.
Escalate immediately as per local CERS protocol.
This protocol is intended to be used by registered and enrolled nurses within their scope of practice and as outlined in The Use of Emergency Care Assessment and Treatment Protocols (PD2024_011). Sections marked triangle or diamond indicate the need for additional prerequisite education prior to use. Check the medication table for dose adjustments and links to relevant reference texts.

- Activate the Adult Sepsis Pathway.
- This protocol authorises nurses to request diagnostics and give medication and fluids as indicated below, in line with the Adult Sepsis Pathway.
- Attempt blood cultures and sampling prior to giving antibiotics, but do not delay treatment.
- For women who are pregnant or less than 6 weeks post partum, use the Maternal Sepsis Pathway. Do not use this protocol.
Repeat and document assessment and observations to monitor responses to interventions, identify developing trends and clinical deterioration. Escalate care as required according to the local CERS protocol.
Precautions and notes
- The absence of fever in elderly patients is frequent. Infection should be suspected in elderly patients who have acute functional decline, including new or increasing confusion, falls, reduced oral intake or change in urinary habits.
Interventions and diagnostics
Pathology
Attempt blood cultures and sampling prior to giving antibiotics, but do not delay treatment.
- FBC, UEC, LFT, glucose, VBG with lactate, CRP
- Blood cultures: take two sets of blood cultures from two separate sites. If patient has a central venous access device (CVAD) in situ, take one set of blood cultures from CVAD, and one set from a peripheral site
- Urinalysis: mid-stream (preferred), clean catch or catheter urine. If positive for nitrites and/or leucocytes send for MC&S. Keep sample refrigerated if transport delayed
- Consider using for specific fever sources: wound swab, sputum culture, stool culture, respiratory viral screen
Fluid resuscitation
Give sodium chloride 0.9% 500 mL IV/intraosseous bolus.
Assess response. Aim for systolic blood pressure 100 mmHg or over.
If ongoing hypotension, repeat once.
Antibiotic management
- Give antibiotics within 60 minutes if:
- patient has probable sepsis with a high risk of deterioration or septic shock
- and a medical or nurse practitioner is unavailable
- and patient is being treated as an emergency patient or as an inpatient as part of a CERS response and presented less than 24 hours ago (designated facilities only).
- Attempt blood cultures and sampling prior to giving antibiotics, but do not delay treatment.
- Document source of infection if known.
Gentamicin
Gentamicin dosing is based on BMI and whether there is known kidney impairment.
If using Gentamicin Dose Advisor in eMR: use the gentamicin dose calculator. It will work out whether to use actual or adjusted body weight.
If no Gentamicin Dose Advisor: use the BMI and adjusted body weight calculator on the webpage.
- BMI under 30: use actual body weight for gentamicin dose.
- BMI 30 and over: use adjusted body weight for gentamicin dose.
Do not give gentamicin if patient has:
- pre-existing significant auditory impairment or vestibular condition
- history of hypersensitivity reaction to aminoglycoside
- myasthenia gravis
- history of aminoglycoside-induced vestibular or auditory toxicity, or first degree relative has history of same.
If the patient has any of the above contraindications, continue to give the other antibiotics and seek advice about gentamicin.
Use the BMI calculator below to determine whether to use actual or adjusted body weight for gentamicin dosing.
Additional antibiotics
Select one:
No known allergies
Give flucloxacillin 2 g IV once only
and if known MRSA or risk of colonisation and/or CVAD in situ:
also give vancomycin 25 mg/kg (actual body weight) IV once only, maximum dose 3 g
Non-severe penicillin allergy
Give cefazolin 2 g IV once only
and if known MRSA or risk of colonisation and/or CVAD in situ:
also give vancomycin 25 mg/kg (actual body weight) IV, once only, maximum dose 3 g
Life-threatening or uncertain penicillin allergy
Give vancomycin 25 mg/kg (actual body weight) IV once only, maximum dose 3 g
Glucose
Measure BGL.
If BGL is less than 4 mmol/L with NO decrease in level of consciousness (Yellow Zone criteria):
- give quick-acting carbohydrate: sugary soft drink, fruit juice or 40% glucose gel, up to 15 g, buccal
- reassess BGL in 15–30 minutes and repeat treatment until BGL over 4 mmol/L
If BGL less than 4 mmol/L WITH a decrease in level of consciousness (Red Zone criteria) OR the patient is unable to tolerate oral intake:
- give 40% glucose gel, up to 15 g, buccally in incremental doses, as tolerated, while establishing IV access
- give 10% glucose 200 mL by IV infusion over 15 minutes, once only
- if delay in IV access, give glucagon 1 mg IM, once only
- reassess BGL in 15 minutes
If the patient is unconscious or peri-arrest:
- give 50% glucose, 50 mL by slow IV injection, once only. Use with caution as extravasation can cause potential serious necrosis
- if delay in IV access, give glucagon 1 mg IM, once only
- reassess BGL in 15 minutes.
Once stabilised, give long-acting carbohydrate and continue to check BGL hourly, or as clinically indicated.
Analgesia
If pain score 1–6 (mild–moderate), give:
- paracetamol 1000 mg orally once only
- and/or ibuprofen 400 mg orally once only.
If severe pain present, give analgesia and escalate as per local CERS protocol.
Nausea and/or vomiting
If nausea and/or vomiting is present, give:
- metoclopramide 10 mg orally or IV/IM once only (over 20 years only)
- or ondansetron 4 mg orally or IV/IM. If symptoms persist after 60 minutes, repeat once, maximum dose 8 mg
- or prochlorperazine 5 mg orally once only or 12.5 mg IV/IM once only
Choice of antiemetic should be determined by cause of symptoms.
Radiology
- If chest thought to be source of infection or source is difficult to determine: CXR
Medications
The shaded sections in this protocol are only to be used by registered nurses who have completed the required education.
Drag the table right to view more columns or turn your phone to landscape
| Drug | Dose | Route | Frequency |
|---|---|---|---|
2 g | IV | Once only | |
2 g | IV | Once only | |
Use actual or adjusted body weight as per BMI guide provided 16–18 years: 18–80 years: 80 years and over: Known kidney impairment and 18 years and over: | IV | Once only | |
1 mg | IM | Once only | |
200 mL | IV infusion over 15 minutes | Once only | |
Glucose 40% gel | 15 g | Buccal | Repeat after 15 minutes if required |
50 mL | Slow IV injection | Once only | |
Ibuprofen H, R | 400 mg | Oral | Pain score 1–10
Once only |
Over 20 years: | Oral/IV/IM | Once only | |
4 mg Maximum dose 8 mg | Oral/IV/IM | Repeat once if required after 60 minutes | |
Oxygen | 2–15 L/min, device dependent | Inhalation | Continuous |
1000 mg | Oral | Pain score 1–10 Once only | |
5 mg | Oral | Once only | |
OR | |||
12.5 mg | IV/IM | Once only | |
500 mL | IV/intraosseous | Bolus Repeat once if required | |
25 mg/kg (actual body weight) Maximum dose 3 g | IV | Once only | |
Medications with contraindications or requiring dose adjustment are marked:
- H for patients with known hepatic impairment
- R for patients with known renal impairment.
Escalate to medical or nurse practitioner.
References
- Clinical Excellence Commission. Adult Blood Culture Guidance. Australia: CEC, NSW Health; 2021 [cited 05 Apr 2024]. Available from: https://www.cec.health.nsw.gov.au/__data/assets/pdf_file/0005/259412/Adult-Blood-Culture-Guidance.PDF
- NSW Health. Australian Medicines Handbook. Australia: Australian Government, NSW; 2022 [cited 13 Apr 2022]. Available from: https://amhonline.amh.net.au.acs.hcn.com.au/
- MIMS Australia. Clinical Resources. Australia: MIMS Australia Pty Ltd; 2022 [cited 2 Feb 2023]. Available from: https://www.mimsonline.com.au.acs.hcn.com.au/Search/Search.aspx
- Roth A, Basello G. Evaluation of fever of unknown origin in adults. London, UK: BMJ Best Practice Group; 2022 [cited 14 Feb 2023]. Available from: https://bestpractice.bmj.com/topics/en-us/375
- NSW Emergency Care Institute. Fever of Unknown Origin. NSW Health, Australia: Agency for Clinical Innovation; 2017 [cited 14 Feb 2023]. Available from: https://aci.health.nsw.gov.au/networks/eci/clinical/clinical-tools/infectious-diseases/fever-of-unknown-origin
- David A, Quinlan JD. Fever of Unknown Origin in Adults. Am Fam Physician. 2022 Feb 1;105(2):137-43.
- Uffen JW, Oosterheert JJ, Schweitzer VA, et al. Interventions for rapid recognition and treatment of sepsis in the emergency department: a narrative review. Clin Microbiol Infect. 2021 Feb;27(2):192-203. DOI: 10.1016/j.cmi.2020.02.022
- Gavelli F, Castello LM, Avanzi GC. Management of sepsis and septic shock in the emergency department. Intern Emerg Med. 2021 Sep;16(6):1649-61. DOI: 10.1007/s11739-021-02735-7
- Dinarello C, Porat R. Pathophysiology and treatment of fever in adults. UpToDate: Wolters Kluwer 2022 [cited 14 Feb 2023]. Available from: https://www.uptodate.com/contents/pathophysiology-and-treatment-of-fever-in-adults
- Daniels R, Nutbeam T, Berry E. Sepsis in adults. BMJ Best Practice BMJ Publishing Group; 2018 [cited 14 Feb 2023]. Available from: https://sthjournalclub.files.wordpress.com/2017/09/245.pdf
- Clinical Excellence Commission. Sepsis Kills Program. NSW Australia: NSW Health; 2022 [cited 10 Feb 2023]. Available from: https://www.cec.health.nsw.gov.au/keep-patients-safe/sepsis/program
- Clinical Excellence Commission. Sepsis Management Plan - Adult Sepsis Pathway. NSW Australia: NSW Health,; 2024 [cited 05 Apr 2024]. Available from: https://www.cec.health.nsw.gov.au/__data/assets/pdf_file/0005/291803/Adult-Sepsis-Pathway.PDF
- Beasley R, Chien J, Douglas J, et al. Thoracic Society of Australia and New Zealand oxygen guidelines for acute oxygen use in adults: 'Swimming between the flags'. Respirology. 2015 Nov;20(8):1182-91. DOI: 10.1111/resp.12620
- Therapeutic Guidelines. Empirical regimens for sepsis or septic shock. VIC, Australia Therapeutic Guidelines Limited; 2021 [cited 14 June 2024]. Available from: https://tgldcdp.tg.org.au.acs.hcn.com.au/viewTopic?etgAccess=true&guidelinePage=Antibiotic&topicfile=sepsis-empirical-regimens&guidelinename=Antibiotic§ionId=toc_d1e437#toc_d1e437
- Therapeutic Guidelines. Management of patients reporting hypersensitivity to penicillins. VIC, Australia Therapeutic Guidelines Limited; 2019 [cited 14 June 2024]. Available from: https://tgldcdp.tg.org.au.acs.hcn.com.au/viewTopic?etgAccess=true&guidelinePage=Antibiotic&topicfile=antimicrobial-hypersensitivity&guidelinename=Antibiotic§ionId=toc_d1e282#toc_d1e282
| Evidence informed |
Information was drawn from evidence-based guidelines and a review of latest available research. For more information, see the development process. |
| Collaboration |
This protocol was developed by the ECAT Working Group, led by the Agency for Clinical Innovation. The group involved expert medical, nursing and allied health representatives from local health districts across NSW. Consensus was reached on all recommendations included within this protocol. |
| Currency | Due for review: Jan 2026. Based on a regular review cycle. |
| Feedback | Email ACI-ECIs@health.nsw.gov.au |
Accessed from the Emergency Care Institute website at https://aci.health.nsw.gov.au/ecat/adult/sepsis