
Ophthalmology
The vital sign for the eye is the measurement of visual acuity (VA). Just as you would measure pulse rate, blood pressure, respiratory rate and O2 saturations for a resuscitation or neurovascular integrity of a limb you must do the VA at the outset. VA measurement must be taken before you do anything or apply anything to the eye.
For information on Eye Trauma - Chemical Burns click here.
Eye Trauma - Chemical Burns
Red Flags
- Once a chemical injury is suspected, you must commence irrigation prior to further history or examination
- Exclude an open globe injury if the mechanism is suspicious (e.g. explosion)
Use nitrous oxide / ketamine if necessary for irrigation.
History Findings
- When did it occur?
- What is the chemical? (e.g. acid / alkali – alkalis are more harmful to the eye).
- Any first aid administered and how soon after the incident?
Examination Findings
- Use topical anaesthesia if necessary
- Visual acuity
- Fluorescein staining - corneal and conjunctival
- Is the cornea clear or cloudy (can you see iris details)?
- The degree of vascular blanching, particularly at the limbus, is proportional to severity of chemical burn (see Figure 1 and 2 for a comparison).
- Evert eyelids – is there any retained particulate matter?

Investigations
- Measure pH using universal indicator paper in the conjunctival fornix (or a cut-off urine dipstick if not available).
- Repeat pH testing after every second litre of fluid.
Important Differentials
- Retained particulate chemical.
- Thermal injury.
- Exclude open globe injury; penetrating or multifactorial injuries. e.g. explosions.
Initial Treatment
IMMEDIATE - EYE IRRIGATION FOR CHEMICAL BURNS
- Instill local anaesthetic drops to affected eye/eyes.
- Commence irrigation with 1 litre of a neutral solution, eg Hartmann’s, N/Saline (0.9%) in an IV giving set on full flow
- Evert the eyelid and clear the eye of any debris or foreign body that may be present by sweeping the conjunctival fornices with a moistened cotton bud.
- Irrigate from 3-5cm above the ocular surface. Ask the patient to look left, right, up and down whilst irrigating.
- A Morgan Lens may only be used AFTER the first litre has been manually irrigated as above. Give more local anaesthetic and then carefully insert the device.
- Review the patient’s pain level every 10 minutes and instil another drop of local anaesthetic as required.
- a. Review after one litre of irrigation.
- If using a Morgan Lens, remove the device prior to review.
- Wait 5 minutes after ceasing the irrigation fluid then check pH in BOTH eyes. Acceptable pH range 6.5-8.5. Compare with unaffected eye’s pH if unilateral injury.
- Consult with the senior medical officer or ophthalmologist and recommence irrigation if necessary.
- Severe burns and alkalis will usually require continuous irrigation for at least 30 minutes with 3 litres of fluid.

Figure 1: Acute Alkali Chemical Injury (mild/moderate)
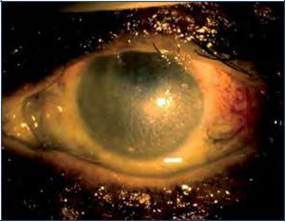
Figure 2: Acute Alkali chemical injury (severe)
Eye Trauma Communication Checklist
Follow ISBAR:
- What is the mechanism of trauma?
- Are you concerned about an open globe injury?
- Is there a history of previous eye surgery or injury?
- What is the visual acuity? (including with pinhole if not 6/6)
- Is there an RAPD?
- What are the findings on slit lamp examination with fluorescein?
- Does the patient have other injuries?
- What treatment has been commenced?
Specific Communication Checklist
- What chemical was involved?
- What irrigation has been done already?
- Have you everted the upper & lower eyelids?
- What is the pH?
Further Information
- The emergency treatment of a chemical injury has far greater impact on the final ocular outcome than any other factor. Prompt and thorough irrigation is critical to avoiding a painful, permanently blind eye in these patients.
- Examples of acids include: toilet cleaner, car battery fluid, pool cleaner.
- Examples of alkalis include: bleach, lime/cement, mortar & plaster, drain cleaner, oven cleaner, ammonia.
- Alkalis saponify ocular tissues and continue to burn deeper into the eye, hence they require more irrigation
- For medicolegal reasons, it is important to document when and how the injury occurred, whether eye protection was present, and any on-site first aid given.

Figure 3: Universal indicator paper
Useful Links
Slitlamp - The movie below runs through basic use and FB removal using the slitlamp. The basic principles of slitlamps are all the same so the best way to see what turning that knob is doing is hold your hand in the beam and watch as you adjust.
This is a piece of equipment which over the years has been sadly misused due to some basic deficiencies in 'knobology' and some principles.
First rule is to leave it how you found it.
Eye Emergency Manual
The Eye Emergency Manual is a quick guide for most ED presentations and is easy to navigate.
The Eye Manual is now available on App for Android and iOS.
Emergency Medicine Cases - outpatient topical anaesthetics for corneal abrasions
- Lateral canthotomy and cantholiyis
- Orbital Fractures
- Something in your Eye